2026-06-08 · insulin resistance, metabolic syndrome, HOMA-IR, weight loss, PCOS, diabetes
Updated 2026-06-13
Written by Nora Kim
Nora Kim is a WeightFAQ staff writer who translates clinical, surgical, and pharmacological weight-loss research into plain-English guidance. She covers the GLP-1 landscape — semaglutide, tirzepatide, and next-generation drugs — alongside bariatric surgery types, post-op nutrition protocols, and revision options. Her articles also address type 2 diabetes remission, cardiovascular risk, PCOS, fatty liver, night eating syndrome, sarcopenic obesity, and how common medications like antipsychotics, statins, and antidepressants affect weight. Nora writes for readers weighing serious clinical decisions and wanting a clear read on evidence, safety, cost, and realistic outcomes.
11 min read
Medically reviewed on Jun 8, 2026
Insulin Resistance and Weight Loss: How to Recognize It and What Actually Reverses It
Quick answer
Insulin resistance is the condition in which muscle, fat, and liver cells stop responding well to insulin, forcing the pancreas to release progressively more to keep blood sugar in range. The result is elevated fasting insulin, easier fat storage, harder weight loss, and over years rising risk of Type 2 diabetes. The four reliable reversal levers, in priority order, are a 5 to 10 percent loss of body weight, resistance plus moderate cardio training, a lower-glycemic and higher-protein eating pattern, and 7 to 9 hours of sleep. Metformin and GLP-1 medications are evidence-backed clinical adjuncts when lifestyle changes are not enough.
What insulin resistance actually is (plain English)
Insulin’s main job is to move glucose out of the bloodstream and into cells — primarily muscle and fat — where it is either burned for energy or stored. When cells become resistant to insulin’s signal, glucose lingers in the blood. The pancreas reads the rising blood sugar and responds by releasing more insulin. For a long time, this compensation works: blood sugar stays in the normal range, but circulating insulin is now chronically high.
High circulating insulin is not a benign state. It promotes fat storage (especially abdominal), blocks the mobilization of stored fat for energy, raises hunger between meals, and over years wears out the pancreas’s beta cells. Eventually compensation fails, blood sugar drifts up, and the picture becomes prediabetes — then Type 2 diabetes. This is also why people with significant insulin resistance often describe weight loss as feeling like swimming upstream: the hormonal environment is actively opposing fat loss before willpower even enters the equation.
The 7 signs you might be insulin resistant
None of these confirm insulin resistance — only blood work does — but the combination of several raises the pretest probability significantly:
- Increased abdominal fat, with a waist circumference above 40 inches in men or above 35 inches in women
- Skin tags on the neck, underarms, or eyelids, or acanthosis nigricans (velvety darkened patches of skin in body folds); painful recurrent boils in the same fold areas may be hidradenitis suppurativa and weight loss, which clusters with insulin resistance through shared adipokine-driven inflammation
- Strong fatigue, sleepiness, or brain fog after carbohydrate-heavy meals (bread, pasta, rice, dessert) — the same central insulin signaling that drives this symptom also underlies the “type 3 diabetes” framing in dementia and weight loss
- Difficulty losing weight despite a reasonable calorie deficit — see the broader troubleshooting in why am I not losing weight
- Sugar or carbohydrate cravings, especially mid-afternoon or after dinner
- A diagnosis of PCOS, a history of gestational diabetes, or a first-degree relative with Type 2 diabetes
- Elevated blood pressure (≥130/85) or low HDL cholesterol on routine labs — the high-triglyceride / low-HDL pattern is the classic insulin-resistant lipid signature; see cholesterol and weight loss for how weight loss moves it, and metabolic syndrome and weight loss for the full 5-marker cluster diagnosis
Two or three of these warrants a conversation with a clinician about formal testing. Five or more is essentially a near-certainty without other explanation.
How insulin resistance is actually tested
There are four main lab approaches, and most standard “metabolic panels” only run the first two — which is why so many cases are missed in the early, most-treatable phase.
| Test | What it measures | Typical reference | Limitations |
|---|---|---|---|
| Fasting glucose | Blood sugar after 8 h fast | <100 mg/dL | Often normal until late-stage insulin resistance — the pancreas masks the problem |
| HbA1c | 3-month average blood glucose | <5.7% | Only rises after glucose itself rises, so misses earlier insulin elevation |
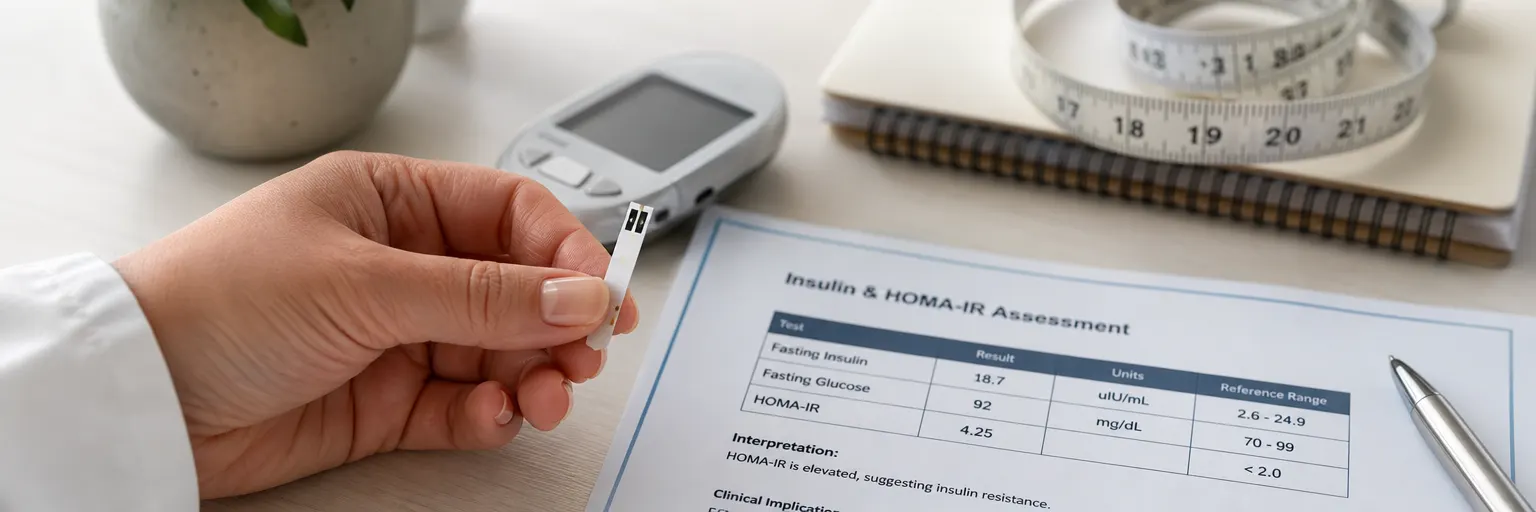
| Fasting insulin | Basal insulin output at rest | <10 µIU/mL (ideal <7) | The single most useful early marker — but rarely ordered on default panels |
| HOMA-IR | Calculated: fasting insulin × fasting glucose ÷ 405 | <1.9 ideal; >2.9 indicates IR | Inherits the limitations of fasting insulin assays; still the best office tool |
If your blood sugar and HbA1c look normal but your symptoms and family history fit the pattern, the practical move is to ask your clinician explicitly for a fasting insulin alongside fasting glucose. Computing HOMA-IR is then trivial. A 75-gram oral glucose tolerance test with insulin levels at 0, 30, 60, and 120 minutes is the gold standard for catching early insulin resistance, but it is not commonly available outside specialist clinics.
The 4 reversal levers (evidence-based)
These are listed in order of effect size in trials, but in practice they reinforce each other and should be deployed together.
Lever 1: Modest weight loss (5 to 10 percent of body weight)
This is the single most impactful lever in the published evidence. The Diabetes Prevention Program showed that a 7 percent weight loss plus 150 minutes per week of moderate activity reduced progression from prediabetes to Type 2 diabetes by 58 percent over three years — outperforming metformin in the same trial. Look AHEAD and the DiRECT remission trial confirmed that visceral and pancreatic fat loss specifically restores insulin signaling well beyond what overall body-weight change would predict. For a starting deficit, see how many calories to lose weight.
Lever 2: Resistance plus cardio exercise
Skeletal muscle is the single largest sink for blood glucose. Resistance training increases GLUT-4 transporter density in muscle, which means each unit of insulin moves more glucose. Even a single bout of moderate-to-hard exercise improves insulin sensitivity for 24 to 48 hours. The practical dose is two to three strength sessions per week plus 150 minutes of moderate cardio, which combines the acute and chronic effects. Start points: strength training for weight loss and walking for weight loss.
Lever 3: Lower-glycemic, higher-protein eating
Replace refined grains and sugar-sweetened beverages with whole grains, legumes, and non-starchy vegetables. Build each meal around 25 to 30 grams of protein, which blunts the post-meal insulin spike compared with carbohydrate-dominant meals, and cap added sugar — see sugar and weight loss for the mechanism. Head-to-head, the Mediterranean and lower-carbohydrate patterns both produce meaningful improvements in fasting insulin and HOMA-IR; adherence matters more than which camp. Honest framing of the lower-carb route is in low-carb and keto diets, and the Mediterranean side is covered in Mediterranean diet weight loss. For readers whose insulin resistance overlaps with chronic joint pain, PCOS, or elevated CRP, the anti-inflammatory diet for weight loss is the same food list under a different framing and consistently improves fasting insulin and HOMA-IR alongside inflammatory markers.
Lever 4: Sleep (7 to 9 hours) and stress management
This is the most under-appreciated lever. A single night of four hours of sleep can produce same-day insulin resistance in healthy adults — the classic finding from Van Cauter and colleagues. Chronic sleep restriction compounds the effect and drives hunger hormones in the wrong direction. Treat sleep as non-negotiable infrastructure rather than a “nice to have.” Stress and cortisol layer on top of this: brief but consistent daily resets outperform sporadic recovery weekends. The full pattern is in sleep, stress, and weight management.
The insulin-resistance plate — what to actually eat
A concrete plate model is easier to maintain than a macro target:
- Half the plate: non-starchy vegetables — leafy greens, broccoli, cauliflower, peppers, zucchini, tomatoes
- One quarter of the plate: lean protein totaling 25 to 30 g — chicken, fish, tofu, Greek yogurt, eggs, lean beef
- One quarter of the plate: high-fiber whole grains or legumes — oats, beans, lentils, quinoa, barley
- One thumb: healthy fat — olive oil, nuts, seeds, avocado
A small but well-replicated trick is meal sequencing: eat the protein and vegetables first, then the carbohydrates. Shukla and colleagues showed that this ordering lowered postprandial glucose and insulin spikes by roughly 20 to 35 percent in people with insulin resistance — without changing what was eaten. It is the cheapest intervention on the page.
Beverages matter independently. Water, unsweetened tea, and black coffee do not raise insulin. Sweetened drinks, fruit juice, and “lightly sweetened” beverages reliably do, and they are one of the most efficient ways to undo the rest of this list.
Medications: metformin, GLP-1s, and what to ask about
Metformin is the most-studied first-line option. It works primarily by reducing hepatic glucose production and modestly improving peripheral insulin sensitivity. The Diabetes Prevention Program saw average weight losses of about 2 to 4 lb on metformin alone — modest but not the main point. With decades of safety data, a generic cost under $10 per month in most pharmacies, and meaningful protection against progression to Type 2 diabetes, it remains a reasonable consideration in higher-risk patients (HOMA-IR consistently above 3, family history, PCOS) who have already started serious lifestyle work. Gastrointestinal side effects are common in the first few weeks; extended-release formulations are usually better tolerated. Insulin resistance can also layer on top of type 1 diabetes and weight loss — sometimes called “double diabetes” — and the REMOVAL trial showed metformin produces a similar modest weight and LDL benefit in that group.
GLP-1 receptor agonists (semaglutide, tirzepatide) produce substantially larger weight loss and dramatic improvements in insulin sensitivity — in the STEP-1 and SURMOUNT-1 trials, fasting insulin and HOMA-IR fell well beyond what weight loss alone would predict, suggesting direct effects on hepatic insulin signaling. They are formally approved for Type 2 diabetes and for obesity, but not for prediabetes or insulin resistance alone, and out-of-pocket cost remains high. If you are weighing the option, see GLP-1 weight loss overview, GLP-1 cost and insurance, and the diabetes-specific framing in diabetes and weight loss. Insulin resistance is also the primary driver of fatty liver disease (NAFLD / MASLD) — the same 5 to 10 percent weight loss that improves HOMA-IR resolves liver steatosis in most patients.
Supplements: what has evidence and what doesn’t
Most “blood sugar support” stacks are marketing. A short, honest pass on what has actual randomized-trial support:
- Inositol (myo-inositol plus d-chiro-inositol, total 2 to 4 g/day) has modest but consistent RCT evidence in PCOS-related insulin resistance — improvements in fasting insulin and HOMA-IR. Reasonable to try; not a substitute for the four levers.
- Berberine has metformin-comparable evidence in small trials for lowering fasting insulin, but product quality control is uneven, drug interactions are real, and long-term safety data are thinner than for metformin. Discuss with a clinician before stacking with other medications.
- Chromium and cinnamon have weak and inconsistent data. They will not hurt you in normal doses; do not expect much.
- Skip proprietary “metabolic reset” stacks. The active ingredients are usually either redundant with the above or unsupported.
The broader landscape is covered in weight loss supplements overview, and the PCOS-specific picture is in PCOS and weight loss.
How long does it take to reverse insulin resistance?
Expectations matter. The realistic timeline, based on the published trial data:
- A single workout: 24 to 48 hours of improved insulin sensitivity
- 2 weeks of consistent exercise plus lower-carbohydrate eating: measurable fasting insulin drop
- 5 to 10 percent weight loss over 3 to 6 months: 30 to 50 percent improvement in HOMA-IR (Diabetes Prevention Program data)
- 15 percent or greater weight loss (DiRECT, GLP-1 therapy, bariatric surgery): possible full remission of Type 2 diabetes in many recent-onset cases
The shorter your duration of insulin resistance, the faster and more complete the reversal. The longer the pancreatic beta cells have been compensating, the more partial — but never zero — the recovery tends to be. The Counterbalance study showed β-cell function recovering within about 8 weeks of a very-low-calorie diet once ectopic pancreatic fat depletes; the type 2 diabetes remission via weight loss guide walks through the twin-cycle timeline in detail.
When to see a clinician
A clinician’s evaluation is the right next step in any of the following situations:
- HOMA-IR consistently above 2.9, or fasting insulin consistently above 10 µIU/mL
- Fasting glucose at or above 100 mg/dL, or HbA1c at or above 5.7 percent
- A family history of Type 2 diabetes plus several of the symptoms above
- A personal history of gestational diabetes or PCOS
- Skin findings (acanthosis nigricans, multiple skin tags) plus central adiposity
- No measurable progress after 4 to 6 months of consistent lifestyle effort
For structured options, medical weight loss programs covers what a typical clinical workup and follow-up plan looks like.
Sources
Sources
- Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin (Diabetes Prevention Program). New England Journal of Medicine (2002).
- Lean MEJ, Leslie WS, Barnes AC, et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomised trial. The Lancet (2018).
- Look AHEAD Research Group. Reduction in weight and cardiovascular disease risk factors in individuals with type 2 diabetes: one-year results of the Look AHEAD trial. Diabetes Care (2007).
- Shukla AP, Iliescu RG, Thomas CE, Aronne LJ. Food order has a significant impact on postprandial glucose and insulin levels. Diabetes Care (2015).
- Wilding JPH, Batterham RL, Calanna S, et al. Once-weekly semaglutide in adults with overweight or obesity (STEP-1). New England Journal of Medicine (2021).
- Jastreboff AM, Aronne LJ, Ahmad NN, et al. Tirzepatide once weekly for the treatment of obesity (SURMOUNT-1). New England Journal of Medicine (2022).